Giving birth is powerful—and so is recovery. Your pelvic floor (the sling of muscles supporting the bladder, uterus, and bowel) works hard through pregnancy and delivery. After birth—vaginal or C-section—those muscles can be stretched, weakened, or injured. The right postpartum plan helps you heal faster, prevent leaks, support your core and back, and get back …
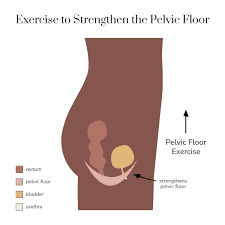
Giving birth is powerful—and so is recovery. Your pelvic floor (the sling of muscles supporting the bladder, uterus, and bowel) works hard through pregnancy and delivery. After birth—vaginal or C-section—those muscles can be stretched, weakened, or injured. The right postpartum plan helps you heal faster, prevent leaks, support your core and back, and get back to the activities you love.
This Algyna guide covers what changes after childbirth, how to start pelvic-floor exercises safely, Lahore-friendly routines, and when to seek help.
Why pelvic-floor care matters after birth
- Urinary incontinence (leaking) is common after childbirth but not “just normal.” A 2021 review found prevalence rises from 24% at 6 weeks to ~32% at 12 months postpartum. Another meta-analysis estimates ~26% overall. Early, structured support lowers risk and symptoms.
- Leading guidelines recommend pelvic floor muscle training (PFMT) as first-line care to prevent and treat postpartum urinary incontinence and pelvic organ prolapse.
- Most women can begin gentle pelvic-floor activation within days of delivery (as tolerated), progressing gradually over the first 6–8 weeks.
Planning your birth or comparing recoveries? Our guide [Normal Delivery vs C-Section in Lahore: Pros, Risks, Recovery & Cost] explains timelines, pain relief, and recovery basics that intersect with pelvic-floor care.
What happens to your pelvic floor during & after birth
- Pregnancy load: Hormones + growing uterus stretch connective tissue; posture changes increase strain on pelvic muscles.
- Vaginal birth: The pelvic floor lengthens substantially as the baby passes. Perineal tears (esp. 3rd/4th-degree) need tailored rehab and protected loading. Avoid high-impact and heavy lifting for ~4–6 weeks, then build up as pain allows.
- C-section: You skip perineal stretching, but the pelvic floor still weakens from pregnancy itself; core/abdominal healing alters pressure and breathing mechanics—so PFMT still matters. Early pelvic-floor activation is safe (after catheter removal and as comfort allows).
Your first 8 weeks: a clear, step-by-step plan
Always follow your clinician’s advice—especially after significant tears, instrumental delivery, or surgical complications. If anything hurts beyond gentle “workout tired,” stop and check in.
Weeks 0–2: Gentle re-activation
- Breathing + awareness (2–3×/day): Lie on your side or back with knees bent. Inhale through the nose, let the belly soften. On a slow exhale, gently lift and draw the pelvic floor (as if stopping urine + wind) for 2–3 seconds, then fully relax. 8–10 reps.
- Bowel care: Stay hydrated, use a stool softener if advised, and exhale on effort to avoid straining (protects stitches and pelvic support).
- Walking: 5–10 minutes, easy pace, building tolerance.
- C-section note: Support your incision when coughing/laughing; start gentle PFMT once the catheter is out and you feel ready.
Weeks 3–4: Foundation strength
- Structured PFMT (Kegels):
- Quick squeezes: Lift-relax for 1 second, 10 reps.
- Endurance holds: Lift and hold 3–5 seconds, relax fully for equal time, 8–10 reps.
- Aim for 3 sets/day. ACOG advises working up toward 10-second holds, three times daily.
- Posture & core: Add heel slides, pelvic tilts, and gentle bridges if comfortable, keeping breath smooth.
- Walking: 10–20 minutes most days.
Weeks 5–8: Strength + function
- Progress PFMT:
- Functional habits: Exhale on exertion (standing with baby, getting off floor), lift with knees, avoid breath-holding.
- Cardio & resistance: Low-impact cycling or brisk walks + light bands/weights; delay high-impact/jumping until cleared and leak-free.
Getting your postpartum plan together? See our [Third Trimester Checklist for Lahore Moms]—use it to line up pelvic-floor physio, support help, and recovery supplies before delivery.
How to do a perfect Kegel (and avoid common mistakes)
- Find the right muscles: Imagine stopping urine and gas at the same time—feel a lift at the front and back.
- No clenching glutes or breath-holding. Keep shoulders/face relaxed; breathe normally.
- Quality > quantity: Full relaxation between reps prevents over-tightness and pain.
- Positions: Start lying, then practice sitting/standing to simulate real life.
- Progression: Build duration slowly toward 10-second holds, 10 reps, 3×/day (your north star, not day-1 goal).
Signs you’re doing too much (or need extra help)
- Leaking worse with activity, heaviness/dragging in the vagina, bulge sensation, or new pelvic pain.
- Pain with penetration or tampon insertion, persistent constipation/straining.
- No improvement in leaks by 12 weeks despite consistent PFMT.
These are cues to see a women’s-health physiotherapist or gynecologist. NICE recommends a multidisciplinary, community-based approach for pelvic-floor dysfunction—ask for referral if symptoms persist.
Lahore-practical lifestyle habits that protect your pelvic floor
- Load management: Stairs and household lifting add up; pace chores, use trolleys, and exhale/lift to spare pressure.
- Bowel rhythm: Fiber-rich Pakistani plates (daal, sabzi, fruit, chia/alsi) + water = easier stools, less straining.
- Feeding positions: If breastfeeding, keep neutral spine and footrest; change positions to reduce pelvic pressure.
- Weight & movement: Gentle walks most days + progressive resistance support continence and back health. A growing research base shows postpartum PFMT reduces odds of incontinence and prolapse.
- Sex & comfort: Use lubricant, go slow, and communicate. If pain persists, request assessment for scar sensitivity or pelvic-floor over-activity.
Want nutrition that steadies energy and supports tissue healing? Many principles from [PCOS Diet Tips in Pakistan: What to Eat for Hormonal Balance] (low-GI carbs, adequate protein, healthy fats) help postpartum recovery too.
When to return to exercise (and which types help most)
- Pelvic-floor & breathing work: immediate/early as tolerated.
- Walking & mobility: ramp up through weeks 1–6.
- Strength training: begin with bodyweight/bands once lochia lightens and wounds are healing; increase load gradually.
- High-impact running/HIIT: wait until leak-free, heaviness-free, and cleared by your clinician/physio—usually after 12+ weeks, individualised.
- After significant perineal tears (3rd/4th degree): avoid high impact and heavy lifting for 4–6 weeks minimum; rebuild under supervision.
Red flags—book a review sooner
- Leaks that aren’t improving after 8–12 weeks of consistent PFMT
- Bulge or persistent heaviness (possible prolapse)
- Severe perineal pain, wound issues, or fever
- Fecal incontinence, new numbness/weakness in legs or saddle area
- Post-C-section incision pain that worsens with gentle breath/core work
Your 12-week recovery roadmap (save this)
Weeks 0–2: breath + gentle PFMT, bowel care, 5–10 min walks
Weeks 3–4: structured PFMT (quick + endurance), 10–20 min walks
Weeks 5–8: progress PFMT (up to 10-sec holds), light bands/bridges, longer walks
Weeks 9–12: add strength circuits (sit-to-stands, rows, dead bugs), low-impact cardio; test light jogging only if leak/heaviness-free and cleared
Evidence you can quote
- UI after birth is common but treatable: ~24% at 6 weeks → 32% at 12 months; targeted PFMT reduces risk and symptoms.
- First-line care: NICE and RCOG endorse regular pelvic-floor exercises for prevention and treatment; start early, progress gradually.
- Start soon: ACOG notes many women can resume activity within days and initiate PFMT immediately postpartum as tolerated.
How Algyna supports your postpartum recovery (Lahore)
At Algyna, we integrate pelvic-floor screening into postpartum checkups, coach you on breathwork & PFMT technique, and collaborate with women’s-health physiotherapists when needed. If symptoms persist, we follow NICE-style multidisciplinary care—tailored to your home routine, modesty needs, and city life.
Expecting soon? Build your plan early with [First Trimester of Pregnancy: What to Expect, Eat & Avoid] then bookmark this pelvic-floor guide for after delivery.
Frequently Asked Questions
Q: Can endometriosis be cured?
A: Currently, there is no guaranteed cure for endometriosis—it is a chronic condition. However, many women achieve excellent symptom relief, maintain fertility, and live full lives with the right treatment plan of surgery, hormones, lifestyle, and ongoing monitoring.
Q: Does severity of pain reflect severity of disease?
A: Not always. You can have minimal visible implants yet experience severe pain, and conversely, extensive disease might produce little discomfort.
Q: Can I conceive if I have endometriosis?
A: Yes—many women with endometriosis conceive naturally. However, the condition can reduce fertility by distorting anatomy, affecting egg/embryo quality, or producing inflammation. Early referral to a fertility-aware specialist improves outcomes. Pakistani data show a high rate of endometriosis among infertile women.
Q: How long should I try medical therapy before surgery?
A: This depends on your symptoms, fertility goals, age, and disease stage. If you have persistent severe pain, fertility issues, or endometrioma >4 cm, your gynaecologist may recommend earlier surgical referral rather than protracted medical therapy.
Q: What lifestyle changes really help?
A: Key changes include a low-GI whole-foods diet, omega-3-rich meals, regular physical activity (especially pelvic-friendly strength and mobility), mindfulness/stress control, good sleep, and avoiding smoking/alcohol (if applicable). These don’t replace medical treatment but improve symptom control and quality of life.
Sign up for free Session!
It’s easy and free!