Post-menopause is a powerful new chapter—one that calls for upgraded self-care rather than slowing down. As estrogen declines, risks for osteoporosis, fractures, cardiometabolic disease, sleep issues, and mood changes rise. The good news? With the right nutrition, bone-loading movement, vitamin D & calcium strategy, and personalized hormone support, Pakistani women can stay strong, clear-headed, and …
Post-menopause is a powerful new chapter—one that calls for upgraded self-care rather than slowing down. As estrogen declines, risks for osteoporosis, fractures, cardiometabolic disease, sleep issues, and mood changes rise. The good news? With the right nutrition, bone-loading movement, vitamin D & calcium strategy, and personalized hormone support, Pakistani women can stay strong, clear-headed, and active for decades.
This guide is for Algyna readers in Lahore and beyond.
Why post-menopause wellness matters (Pakistan context)
- In a study of post-menopausal women in rural Pakistan, 42% had osteopenia and 29% had osteoporosis, with mean calcium intake only ~346 mg/day—less than half of recommended intakes. Vitamin D deficiency and low calcium intake were key contributors to poor bone status.
- Broader estimates suggest ~9.9 million people in Pakistan live with osteoporosis—7.2 million are women.
- Vitamin D deficiency is widespread: one national review estimates ~63% of Pakistani women are vitamin-D deficient (and another analysis highlights particularly high deficiency among pregnant women). Deficiency worsens bone loss and fracture risk.
- Regionally, Asia is on course to bear over half of the world’s osteoporotic hip fractures by 2050—a reminder that prevention today protects independence tomorrow.
- Bottom line: Post-menopause is the time to proactively protect bones, muscles, heart, and mood—with changes that fit Pakistani food culture, home routines, and city life (Lahore traffic, limited outdoor spaces, busy family dynamics).
What changes after menopause?
- Estrogen falls → bone resorption outpaces bone formation → accelerated bone loss (first 5–7 years), higher fracture risk.
- Body composition shifts → more central fat, lower lean mass (sarcopenia risk).
- Vasomotor & urogenital symptoms → hot flashes, night sweats, vaginal dryness.
- Sleep & mood → more awakenings, anxiety/low mood for some women.
- Metabolic health → insulin resistance, blood-pressure and lipid changes.
These are modifiable. Start with food and movement, then layer in targeted supplements and, when appropriate, medical therapy.
Nutrition blueprint for Pakistani post-menopausal women
Your daily anchors
- Calcium: target 1,000–1,200 mg/day (diet + supplement, per your doctor).
- Vitamin D: dose guided by blood levels; deficiency is common locally.
- Protein: ~1.0–1.2 g/kg/day (higher if medically suitable) to maintain muscle and bone.
- Omega-3s & anti-inflammatory foods: fish, walnuts, flax; generous haldi/ginger/garlic.
- Magnesium + vitamin K (esp. K2): support bone matrix and calcium handling.
Lahore-friendly plate ideas
- Breakfast: daliya with milk + chopped almonds & figs or 2 eggs + sautéed saag + 1 small multigrain roti.
- Lunch: grilled fish/chicken + mixed sabzi + bowl of salad + small brown rice.
- Snack: dahi (yogurt) + chia seeds or roasted chana/makhanay.
- Dinner (earlier): daal + seasonal veg (gobi/bhindi/tori) + multigrain roti.
- Hydration: water, infused water; limit sugary drinks.
- Tea/coffee: enjoy, but avoid excess (high caffeine can nudge calcium loss).
Smart swaps (Pakistani pantry)
- Atta mix: whole-wheat + barley (jau) or chana flour for more fiber/minerals.
- Cooking fats: mustard/canola/olive oil; avoid re-using oil.
- Sweet tooth: dates or fruit + nuts instead of mithai/very sweet biscuits.
Want hormone-smart habits that also steady energy? See [PCOS Diet Tips in Pakistan: What to Eat for Hormonal Balance]—many low-GI, protein-forward principles help after menopause too.
Bone health: screen early, train wisely
1) Screening & labs
- Ask your doctor about a DEXA scan (baseline at or soon after menopause, earlier with risks: prior fracture, long-term steroids, early menopause).
- Check 25-OH vitamin D, calcium, and related markers; correct deficiencies (very common locally).
2) Bone-loading movement (home-ready)
- Weight-bearing cardio: brisk walking or safe indoor laps 30 mins, 5 days/week.
- Resistance (2–3×/week): chair squats, wall push-ups, hip bridges, band rows (2–3 sets x 8–12 reps).
- Balance drills: single-leg stands, tandem walk along a hallway.
- Posture & mobility: thoracic extensions, hip flexor stretches.
(Always clear new exercise with your clinician—especially if you already have low BMD or joint issues.)
3) Fall-proof your home
- Declutter floors, add night lights, wear supportive footwear indoors, keep a grab-bar near steps if needed.
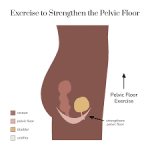
Planning pelvic-health support too? Many women ask about delivery recovery and pelvic floor even years later; [Normal Delivery vs C-Section in Lahore: Pros, Risks, Recovery & Cost] includes pelvic-floor basics you can still apply.
Hormone therapy & non-hormonal supports—what’s safe?
- Menopausal hormone therapy (MHT/HRT) is the most effective treatment for hot flashes and genitourinary symptoms and prevents bone loss and fractures when appropriately prescribed. The benefit–risk profile is most favorable for healthy women <60 years or within 10 years of menopause; decisions should be individualized and re-evaluated regularly.
- If systemic HRT isn’t suitable, low-dose vaginal estrogen (or alternatives) can relieve dryness and support urogenital health.
- Lifestyle first remains key: even with HRT, prioritize nutrition, vitamin D/calcium sufficiency, resistance training, sleep, and stress care.
New to Algyna? Start with our reader-favorite [First Trimester of Pregnancy: What to Expect, Eat & Avoid] if your daughter or daughter-in-law is expecting—useful to support women across life stages.
30-Day Lahore-friendly action plan
Week 1: Foundations
- Book a bone-health consult (discuss DEXA + vitamin D).
- Start 10–15 minutes of morning sunlight (face/arms, where culturally/practically possible).
- Begin 20-minute walks after lunch or Asr; add 5 minutes of deep breathing before bed.
Week 2: Protein & strength
- Hit protein with every meal (eggs, chicken, fish, daal + roti combo).
- Add 2 resistance sessions (chair squats/wall push-ups/hip bridges/band rows).
- Track calcium sources; consider low-sugar dahi snack daily.
Week 3: Upgrade micronutrients
- Include leafy greens, sesame/til, almonds, and small fish (if eaten) for calcium + K.
- Discuss vitamin D dosing with your clinician (deficiency common).
- Reduce late-night meals and screens to protect sleep.
Week 4: Review & personalize
- Re-check symptom log (hot flashes, sleep, aches, mood).
- With your doctor, consider HRT if symptoms remain disruptive and you’re a good candidate—especially if within 10 years of menopause.
- Join a walking group/WhatsApp circle for accountability.
Three evidence points you can quote
- Pakistan bone health gap: Among post-menopausal women in a rural cohort, 42% had osteopenia and 29% osteoporosis, with ~346 mg/day mean calcium intake and frequent vitamin-D deficiency.
- Scale of the problem: ~9.9 million Pakistanis have osteoporosis—7.2 million women—underscoring the need for screening and prevention.
- Regional urgency: By 2050, >50% of the world’s hip fractures are projected to occur in Asia, so early prevention in Pakistan is essential.
Quick myth-busting
| Myth | Reality |
| “Bone loss slows on its own after menopause.” | Bone loss accelerates in the early post-menopause years—plan proactively. |
| “HRT is unsafe for everyone.” | For healthy women <60 or within 10 years of menopause, the benefit–risk profile is favorable when individualized; HRT reduces vasomotor symptoms and prevents bone loss/fractures. |
| “Vitamin D isn’t an issue in sunny Pakistan.” | Deficiency is common due to indoor living, clothing, diet; testing and treatment matter. |
The Algyna approach (Lahore)
At Algyna, we combine evidence-based gynecology with practical lifestyle care:
- Bone-health assessment (DEXA referrals, vitamin D/calcium strategy)
- Pakistani-friendly nutrition coaching (multigrain swaps, daal+protein pairings)
- Home-based resistance and balance sessions
- Symptom-guided HRT counseling (when appropriate), plus non-hormonal options
- Sleep and stress-care routines you’ll actually keep
Ready for a personalized plan? Bring a 2-week food/symptom log to your consult—we’ll tailor the next steps.
Frequently Asked Questions
Q: When should I get a DEXA scan?
A: Talk to your gynecologist about a baseline around or soon after menopause (earlier if you’ve had fractures, long-term steroids, or early menopause). Screening detects silent bone loss before a disabling fracture.
Q: How much calcium and vitamin D do I need?
A: Many post-menopausal women benefit from 1,000–1,200 mg/day calcium (diet ± supplement) and vitamin D individualized to blood levels; deficiency is common in Pakistan and should be corrected under medical guidance.
Q: Is HRT right for me?
A: HRT is the most effective option for hot flashes/vaginal symptoms and helps prevent bone loss. It is most favorable for healthy women under 60 or within 10 years of menopause, with shared decision-making and periodic re-evaluation.
Q: Can I improve bone density without HRT?
A: Yes—adequate calcium/vitamin D, resistance + weight-bearing training, and fall-prevention are powerful. If osteoporosis is diagnosed, your clinician may recommend medications (e.g., bisphosphonates, SERMs). Lifestyle remains the foundation.
Q: I cover up and work indoors—can I still get vitamin D from the sun?
A: You might not get enough. That’s why testing and supervised supplementation are important for Pakistani women.
Sign up for free Session!
It’s easy and free!